
![]() As part of the Academic Path of the II Level International Master ISSMM, whose contents and whose purposes are available online on the website ISSMM – University Tor Vergata (here), in addition to course lectures, the Governing Council has designed and organized various other events such as Conference, Seminars, Workshops, Study Days, taught by recognized High Professionalism and Experience Speakers and sometimes in synergy with Organizations / Research centers, public-private, civil-military institutions to pursue the objectives of Excellence of said Master. (see video)
As part of the Academic Path of the II Level International Master ISSMM, whose contents and whose purposes are available online on the website ISSMM – University Tor Vergata (here), in addition to course lectures, the Governing Council has designed and organized various other events such as Conference, Seminars, Workshops, Study Days, taught by recognized High Professionalism and Experience Speakers and sometimes in synergy with Organizations / Research centers, public-private, civil-military institutions to pursue the objectives of Excellence of said Master. (see video)
Category Archives: Telemedicine
Tele-health & Tele-medicine: From Saying to Doing.
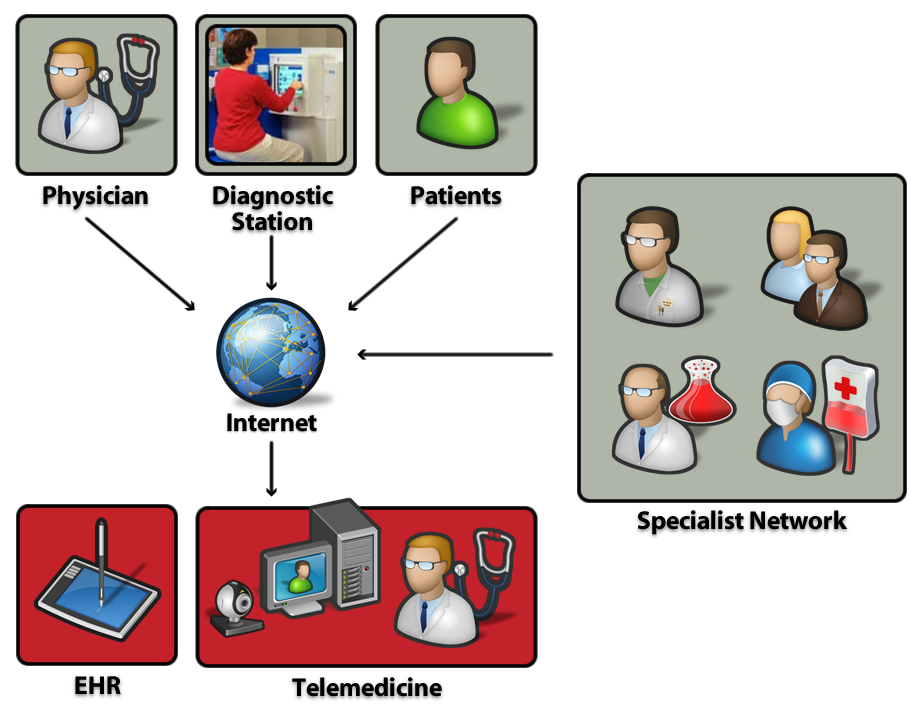 The Information Technology Executives Club of Rome – CDTI, in the spirit of contributing with the skills and experience of its members in the development of the country, involving multidisciplinary professional such as doctors, researchers, entrepreneurs, professionals and IT executives, created an Health Working Group (HWG), which identified the Telemedicine as a fundamental theme for the development of E-Health, also analyzing its recently issued operational guidelines, to synthesize in a single document the information elements for the development of services and the rationalization of costs by the use of information technology.
The Information Technology Executives Club of Rome – CDTI, in the spirit of contributing with the skills and experience of its members in the development of the country, involving multidisciplinary professional such as doctors, researchers, entrepreneurs, professionals and IT executives, created an Health Working Group (HWG), which identified the Telemedicine as a fundamental theme for the development of E-Health, also analyzing its recently issued operational guidelines, to synthesize in a single document the information elements for the development of services and the rationalization of costs by the use of information technology.
The working group, considering that,
- Medical Care needs to address the challenges of aging and chronic disease and that the concept of health has evolved into the concept of well-being, and, as such, requesting improvement in quantity and quality of personalized services;
- the reorganization of the Medical Care has not yet included in a systemic way those innovative telematic services that would allow a rationalization and saving resources;
- The addresses of government and recent operational guidelines agreed by the Conference State – Regions and issued by the Ministry of Health, involve the expansion of the territory with a smaller number of hospitals more and more advanced, technologically advanced, dedicated to pathologies high complexity;
and in consideration that the intensive use of information technology and telecommunications (ICT) as key instruments to allow the sharing of information between the various sectors of health and social component without physical travel, the HWG decided to engage himself in the development of a white paper “Telemedicine: from saying to doing.”
This document, which was made public on the occasion of the CDTI September 16, 2014 Seminar in Rome, contains proposals for a concrete and competent support to the “government strategy” for the deployment of telemedicine services in the territory, recognized as an important tool for care and assistance in integration of existing health and social services, effective for cost reduction and increase of services, and also the engine of new jobs in the market.
After years of experimentation isolated, often undertaken voluntarily and dismissed before putting a system on a large scale, a number of national and international experiences have shown that the modern Telemedicine, if programmed in a timely manner in accordance with the more general strategies for improving the quality and efficiency of the health system, is now able to offer significant support to the actions of change in health care systems and proves sustainable in the medium to long term.
Source: Club Dirigenti Tecnologie dell’Informazione di Roma – www.cdti.org
Electronic medical assets and records reduce delays in treatment and enhance healing.
12,681
Battlefield medicine has advanced significantly since the days when surgeons used whiskey as an anesthetic, and in the last year several new technologies have rolled out to deployed soldiers facing physical or psychological disorders. The U.S. Army program responsible for fielding software and the hardware on which it resides is pushing the cutting edge of diagnostics and treatment to the tip of the spear. Personnel hope the effort will save lives and limbs not only by treating injury or illness, but also by keeping troops off the road in war zones.
The Army’s Medical Communications for Combat Casualty Care (MC4) has the service’s Title 10 responsibility to field, sustain and maintain a joint software applications suite for combat medicine. The MC4 is the far-forward Army system used to capture health care information. Applications are developed by the Military Health System and provided to the various military services, which are responsible for placing them into their individual systems. The MC4 integrates the apps into hardware, adding Army-unique systems and apps, and then fields the packages to operational forces. “Army medical units don’t have hardware unless we provide it,” explains Lt. Col. William Geesey, USA, the MC4 product manager.
Since beginning field operations in 2003, the MC4 has enabled the capture of more than 16.5 million electronic patient encounters in combat zones. The system-of-systems also has trained 61,000 medical staff and commanders and fielded 49,000 systems to 750 units with medical personnel. This includes Army National Guard and Reserve units as well as active components in 19 countries.
One of the systems fielded by the MC4 in the last year centers on tele-behavioral health. It leverages commercial technologies available in theater to create a videoteleconference capability that enables mental health providers to conduct private consultations with soldiers at far forward operating bases who otherwise might go untreated. An Army division with as many as 10,000 to 15,000 troops spread over multiple locations may have only one psychiatrist assigned to it, meaning that either that single physician has to travel to all those places to provide treatment, or soldiers have to travel to the doctor’s location. Either way, troops traverse treacherous terrain. Through the videoteleconferences, care can be provided more quickly and safely.
Col. Geesey says that information coming in from the field reports that 70 percent of the doctor-patient interactions resulting from the new technology would never have occurred without it. “When you’re at a forward operating base, you’re not going to get onto a road that’s dangerous or get on an aircraft to go see a psychiatrist who’s far away,” he states. With the system, soldiers can visit their local medical facility and have a consult with a mental health provider in another place.
Also completed in 2011, the MC4 fielded a mild traumatic brain injury (mTBI) documentation capability and assessment tool. When a solider is exposed to an improvised explosive device (IED), a medical provider can administer a battery of tests to determine injuries. The results are documented in the electronic record that is at the heart of the MC4. Through this digital trail, all the medical care soldiers receive from the time they enter service through the rest of their lives is captured in one database accessible by military and Veterans Affairs Department (VA) health care providers. The result is faster diagnosis and treatment as well as an elimination of repeated tests or procedures. With the mTBI information recorded, medical practitioners can access the data if a soldier affected by a blast develops problems in the future.
In addition to its immediate application, the mTBI tool also helps feed research and development efforts by providing data on thousands of soldiers affected by IEDs. “You can use that for developing treatments and also materiel solutions,” Col. Geesey says. Overall, he explains, MC4 systems are designed to focus comprehensively on the entire soldier. The mTBI and telehealth initiatives have a focus on the effects of IEDs on the human body, responding to a number of studies showing a correlation between higher incidences of IED exposure and elevated depression rates.
Another recent MC4 update involved the fielding of a medical logistics capability to Army combat support hospitals for the first time. A hospital at Camp Dwyer, Afghanistan, became the premier facility in Southwest Asia to employ this Defense Medical Logistics Standard Support system, which serves as an automated medical logistics inventory management and property accountability tool. The fielding team consisted of MC4 and 6th Medical Logistics Management Center personnel.
The MC4 is interested in taking advantage of the many Army and personal technologies available in the field and is in the midst of an initiative to make online training courses available on smart devices. The content includes interactive video and constantly updated documentation. Though the Army is still in the process of officially acquiring and fielding smart devices to soldiers, Col. Geesey explains that by his estimation based on personal observations and the observations of others who have deployed, the vast majority of soldiers carry their own laptops and smartphones in theater. Through these, they can access the latest MC4 resources. The initial version of the MC4 guide was available only in a PDF format accessible on computers via Army Knowledge Online.
Lt. Col. T. Sloane Guy IV, USA (right), chief of surgery with the 47th Combat Support Hospital, Mosul, Iraq, reviews an image of a patient’s chest with specialists located at Brooke Army Medical Center at Fort Sam Houston, Texas. The operation showcased technology that connects deployed medics with experts back in the United States to provide the best possible medical care in the field.
Moving forward, the MC4 plans to take the Army’s tele-behavioral health program and expand it to demonstrate a broader telehealth capability. During the next several Network Integration Evaluation events—the Army’s new method for evaluating and more rapidly fielding necessary technology assets into the field—MC4 personnel are scheduled to demonstrate that the concept can help medical specialists address the concerns of forward-deployed soldiers who lack access to such expertise at their locations. “The idea is to reduce the amount of time soldiers have to travel or take to be evaluated,” Col. Geesey explains.
Already, the MC4 system was instrumental in a one-in-a-million surgery that helped an Iraqi receive the medical assistance he required. The surgeon in theater was able to consult via a videoteleconference with a specialist at Brooke Army Medical Center in Texas to conduct the procedure and save the man’s life. This telesurgery mentor initiative was led by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technical Research Center.
Col. Geesey says the MC4’s telehealth efforts eventually could have applications across the Army, but for now the work is focused on units that have the fewest medical providers and specialists assigned to them. “MC4 really offers a tool that enables a provider to deliver better health care,” he explains. “It’s not a clinically invasive device that heals soldiers. What we primarily do is leverage emerging commercial technologies to support the deployed service member.” This support includes laboratory results, pharmaceuticals and X-rays. Keeping all the information collected electronically means that in emergency situations, personnel do not have to worry about sending the right paperwork with patients, and it eliminates situations where information may arrive too late or not at all.
Having information stored and available electronically throughout soldiers’ lifetimes creates advantages in non-emergency situations as well in immediate life-or-death incidents. For example, a soldier who breaks his ankle while in service may require VA compensation for problems the injury causes later in life. With the captured information, everyone can validate a claim more easily. Access to the information also helps protect troops from overexposure to radiation because of unnecessary X-rays and informs doctors about how often patients have been seen for certain complaints regardless of where in the military they sought care or who provided it.
In addition, the technology can capture what vaccines and medicines soldiers received in theater and how those could be affecting them now. With enough statistics like those, researchers could make links between exposures and conditions. “For uniformed troops, it helps increase continuity of care,” Col. Geesey explains. “It allows [medical providers] to see all of soldiers’ prior medical history and have a better picture of what potentially is impacting them.”
The MC4 soon could have even more pieces of data to manage if MRI devices are fielded in theater. Though the office is not responsible for moving the devices to forward locations, it would serve as the information technology enabler for synching the medical images from the machines with soldiers’ electronic medical records.
The medical systems program has an initiative underway to integrate its technology into signal networks in theater. “The bottom line is we rely on the signal community to provide the communications for us to move the information around the battlefield and to [the continental United States] CONUS,” Col. Geesey says. “Sometimes what we find in theater is that the medical guy will go to the signal guy, and the signal guy says ‘That’s medical. I don’t touch that.’ We’ve been working with signal leadership to resolve these issues.”
Another important player in MC4 efforts is industry. Col. Geesey explains that his organization looks to partner with the private sector to leverage current and emerging technologies. His message for industry is similar to many in the military, but the officer emphasizes that he requires solutions that are “commercial standards, open source, open architecture and nonproprietary. Sell me a solution; don’t sell me hardware. Don’t tell me this is the device I need to do something. Give me the capability that supports the mission I’m trying to meet.”
WEB RESOURCES
MC4: www.mc4.army.mil
Military Health System: www.health.mil
Telemedicine and Advanced Technical Research Center: www.tatrc.org